研究背景:
青光眼是因视网膜神经节细胞(RGCs)及其轴突进行性变性而导致不可逆性失明的主要原因。眼内压(IOP)升高是其主要危险因素,但即使降低眼内压(IOP)后,青光眼患者中仍有很大比例会出现视网膜神经节细胞(RGC)丢失,仍会继续出现视力丧失。这一现象凸显了研发可增强视网膜神经节细胞对高眼压耐受能力的治疗手段的必要性。线粒体功能障碍是连接高眼压与视网膜神经节细胞变性的关键机制。本研究旨在探究一种新型高密度芳香肽HDAP2(可结合心磷脂以稳定线粒体膜)能否对DBA/2J小鼠模型中的视网膜神经节细胞发挥保护作用。
方法:
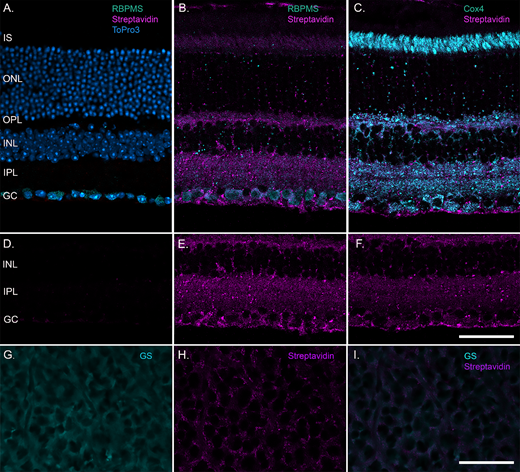
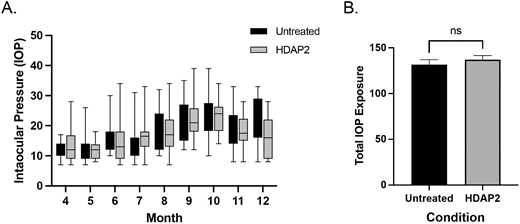
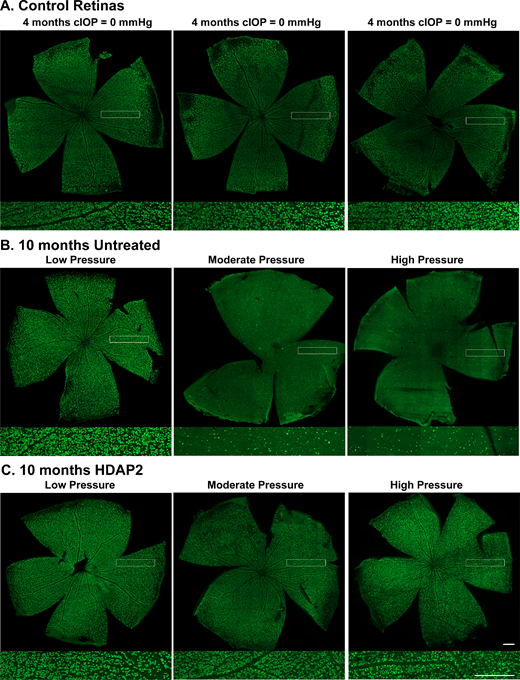
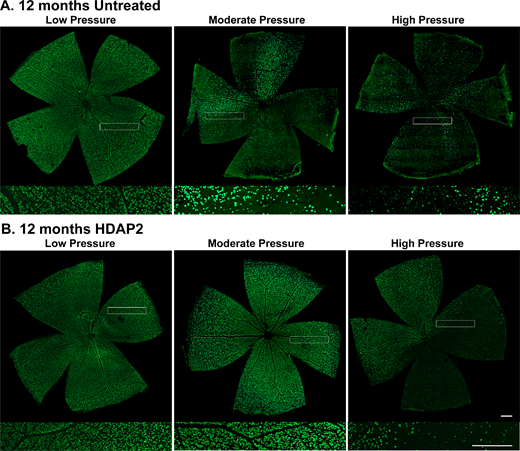
4 月龄 DBA/2J 小鼠开始给予新型多肽HDAP2(3 mg/kg,腹腔注射,隔日 1 次),连续给药 8 个月。每月采用大小鼠专用回弹式眼压计Tonolab(Icare Finland Oy,芬兰赫尔辛基)监测眼压(IOP)以记录眼压暴露情况。通过视网膜铺片 RBPMS 染色细胞计数、以及甲苯胺蓝半薄切片视神经轴突计数,评估视网膜神经节细胞(RGC)存活情况。
新型多肽 HDAP2 由商业公司合成(GenScript, Piscataway, NJ, USA),经高效液相色谱(HPLC)及质谱法鉴定,其纯度>96%。该多肽可靶向线粒体,并与线粒体内膜上的心磷脂结合,在氧化应激状态下维持线粒体膜电位。
结果:
在眼压暴露水平相近时,HDAP2 处理组视网膜的视网膜神经节细胞(RGC)数量较未处理组高出约 49%(P = 0.0063;F (2, 59) = 5.524)。在轻度眼压暴露时,HDAP2 可多保留 58% 的 RGC;在高眼压条件下,RGC 存活率较未处理组提高 180%。Kaplan–Meier 分析显示,HDAP2 使发生严重 RGC 丢失的眼压阈值提高了 29 mmHg(毫米汞柱),并使严重 RGC 变性的发生风险降低至原来的 1/4.6。处理组视网膜的视神经轴突也得到良好保护,轴突形态与对照组无明显差异。各处理组间轴突大小分布无显著改变,提示 HDAP2 对不同亚型 RGC 的保护作用相近。
图一
图二
图三
图四
结论:
本研究结果具有重要的临床意义。目前青光眼的治疗策略几乎完全聚焦于降低眼压,但许多患者即使眼压得到良好控制,仍会持续发生视力丧失。标准治疗通常仅能使眼压降低 20%~30%,相当于降低约 4~8 mmHg⁴²⁻⁴⁴。
与之相比,HDAP2 可将发生严重视网膜神经节细胞(RGC)丢失的阈值提高 29 mmHg。这种保护作用在幅度上与传统治疗相当,但其机制是通过直接神经保护实现,而非降低眼压。
该效应可使严重视力损伤的风险降低 4.6 倍(46.2% 降至 15.6%),这一差异具有明确的临床价值。
在不同眼压暴露水平下,HDAP2 均可同时保护视网膜神经节细胞(RGC)与轴突,并提高对眼内压(IOP)的耐受能力。上述结果提示,HDAP2 可作为降眼压治疗的补充手段,适用于正常眼压性青光眼及难治性青光眼。